1 in 4 Brain-Injury Patients Diagnosed as Unconscious Followed Commands on fMRI, Multicenter Study Found
A prospective study of 353 adults with disorders of consciousness at six international centers detected command-following on brain imaging in 60 of 241 patients (25%) whose bedside examination found no observable response. Published in the New England Journal of Medicine in August 2024, the findings mean 1 in 4 patients clinically diagnosed as comatose, vegetative, or minimally conscious were covertly performing cognitive tasks that their doctors could not detect.
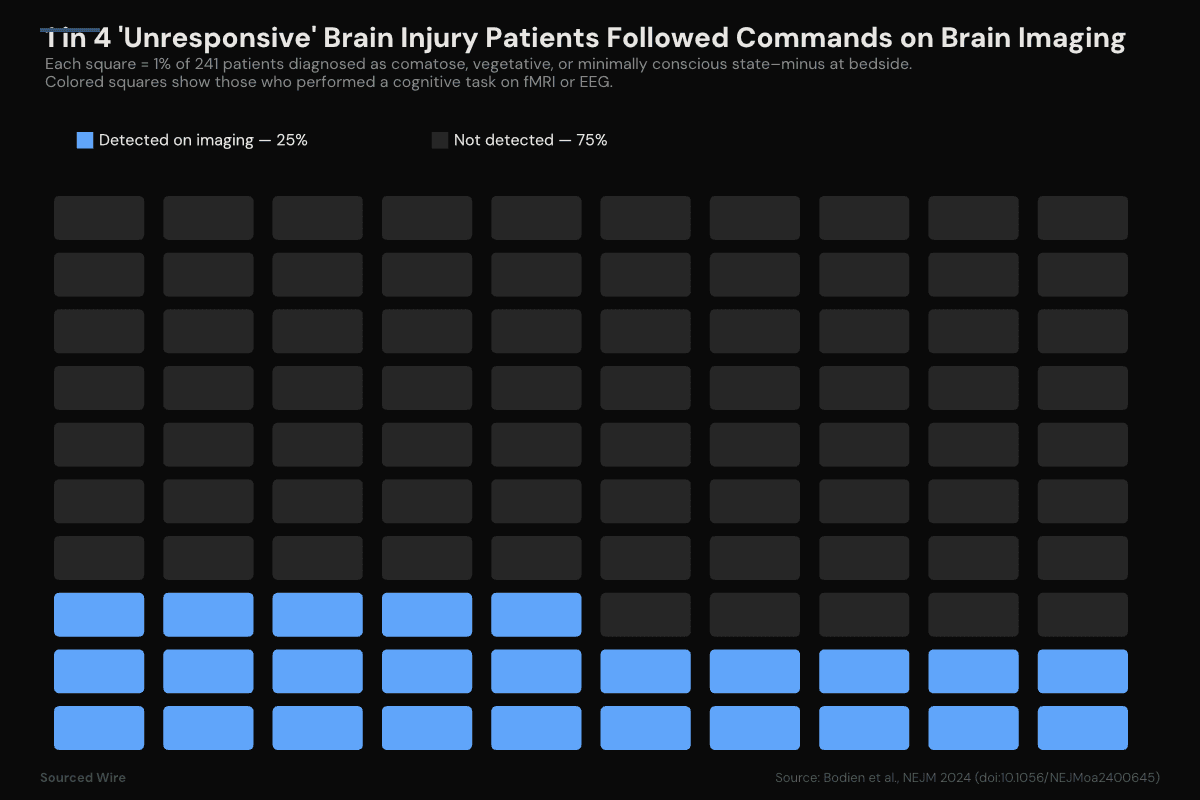
Of 241 adults with severe brain injury and no observable response to verbal commands at bedside, 60 — approximately 25% — performed a command-following cognitive task on functional MRI or EEG, according to a prospective cohort study published in the New England Journal of Medicine in August 2024.
The study, led by Yelena G. Bodien of Massachusetts General Hospital and Harvard Medical School with collaborators from six international centers in the United States, United Kingdom, Belgium, France, and Canada, is the largest systematic investigation to date of a phenomenon known as cognitive motor dissociation — when a patient can respond to commands on brain imaging despite appearing, by every bedside test, to be unconscious.
The finding
The cohort consisted of 353 participants assessed with the Coma Recovery Scale–Revised (CRS-R) and at least one command-following paradigm on functional MRI or EEG within seven days. The median age was 37.9 years. Brain trauma was the etiology in 50% of cases. The median time from injury to assessment was 7.9 months, with 25% assessed within 28 days of injury.
Among the 241 participants with a bedside diagnosis of coma, vegetative state, or 'minimally conscious state–minus' — the three categories that define 'no observable response to commands' under the CRS-R — cognitive motor dissociation was detected in 60 patients (25%). Of those 60, eleven were identified on fMRI only, thirteen on EEG only, and thirty-six on both techniques.
The authors wrote in their conclusion: 'Approximately one in four participants without an observable response to commands performed a cognitive task on fMRI or EEG as compared with one in three participants with an observable response to commands.' The 38% figure for the 'observable response' group — who were judged responsive at bedside — is striking in the opposite direction: 62% of those patients, despite appearing responsive clinically, did not produce an imaging signal on the task, suggesting the two assessment modalities test related but distinct capacities.
Cognitive motor dissociation was more common in younger patients, in those further from the time of injury, and in those whose injury was traumatic rather than hypoxic or other etiology.
What the task actually measures
The imaging tasks rely on mental imagery: patients are asked, for example, to imagine playing tennis, or to imagine walking through their house. These distinct imagined movements produce distinct patterns of activation in the supplementary motor area and the parahippocampal gyrus that functional MRI and quantitative EEG can reliably detect. A patient who is asked to 'imagine playing tennis when you hear a tone' and does so repeatedly on cue is following commands — even if the only evidence of the response is a change in blood oxygenation deep in the brain.
The technique has been validated in the neurological literature since 2006, when Adrian Owen's group first demonstrated that a behaviorally vegetative patient could generate these same activation patterns on command. The Bodien paper established that this is not a rare anomaly: it is a feature of 1 in 4 patients whose bedside examination cannot detect consciousness.
Follow-up in acute care
In March 2026, Bodien and colleagues at Mass General's Center for Neurotechnology and Neurorecovery published a follow-up in the Journal of Neurotrauma examining 55 patients with acute severe traumatic brain injury in the intensive care unit. Of 45 patients with six-month outcome data, 10 died — all from withdrawal of life-sustaining treatment, and all of the patients who died were not behaviorally following commands on the bedside CRS-R at the time of the decision. Cognitive motor dissociation was detected on EEG in 6 of 34 (18%) patients without bedside command-following in that cohort.
The acute-care numbers are smaller and the study does not establish that any of the patients whose families chose withdrawal of care had covert consciousness. But the authors note that behavioral assessment at the time end-of-life decisions are typically made 'may not fully capture a patient's underlying level of consciousness.'
Study limitations
The 2024 cohort was not population-based; it was a convenience sample assembled across six research centers with access to advanced imaging, and the results are therefore not directly generalizable to community hospitals that lack the protocols and equipment to run these paradigms. The task-based imaging protocols also require specialized expertise in paradigm design and signal analysis — they are not a turnkey bedside test. The authors called for prospective validation and work toward clinical implementation.
Funding for the Bodien et al. 2024 study came from the James S. McDonnell Foundation.
Citations
- Bodien YG, Allanson J, Cardone P, et al. 'Cognitive Motor Dissociation in Disorders of Consciousness.' N Engl J Med. 2024 Aug 15;391(7):598-608. doi:10.1056/NEJMoa2400645. PMID: 39141852.
- Bodien YG, Fecchio M, Gilmore N, et al. 'Multimodal Biomarkers of Consciousness in Acute Severe Traumatic Brain Injury.' J Neurotrauma. 2026 Mar;43(5-6):373-386. doi:10.1177/08977151251377469. PMID: 41182259.